Cancer is a worldwide issue accounting for millions of deaths every year, but through research on reliable treatment of brain tumors, safer and less harmful cancer therapy can be utilized for tumor treatment independent of its location. Proton-based treatment of brain tumors demands a precise stopping range and a minimal transverse spread of the protons to not damage any healthy brain tissue. Today's radiation therapy can unintentionally harm nearby cells, which may become fatal in the context of the brain, this implies that there is a need for a safer method for brain tumor treatment. The characteristics of proton-based cancer therapy are here investigated in an attempt to solve this issue in the context of a cyclotron acting at a kinetic energy of 230 MeV. The performed simulations suggest that proton therapy is a valid approach for treatment of brain tumors, the minimal harm on healthy brain tissue may eliminate side effects and save lives.
1. Introduction
This paper regards the treatment of cancer developed in the human brain, and the specific cancer therapy considered is based upon the usage of protons. Treatment of brain tumors demands highly accurate and careful methods in order to not damage any healthy cells outside the tumor. This puts pressure on the facility used for the proton beam, and it is important to accurately focus the protons at the tumor, with a stopping range that minimizes the radiation dose to healthy cells.
The topic of cancer therapy, in general, is in need of a lot more research and knowledge than there is today. Cancer is the second most common cause of death in the world, and it accounts for about 10 million deaths a year (i.e. cancer is roughly the cause of every 6th global death).[1][2] Furthermore, the extra care needed for treatment of brain tumors could, in turn, be applied for the treatment of tumors in other areas, this emphasizes the fact that if reliable tools are developed to treat tumors in sensitive areas, it will contribute to a safe and non-harmful way of treating cancer in general.
For malignant brain tumors, it is common to use chemotherapy, however, this kind of brain tumor still has a high mortality, even when using today's drugs. Although nonmalignant brain tumors are often effectively treated using radiation therapy, it is likely to harm healthy brain tissue and cause mild to deadly side effects, commonly referred to as radiation necrosis. This subsequent necrosis, due to the high radiation exposure, may include: headaches, seizures, and (occasionally) death. These are the same signs of having a brain tumor, i.e. it may be difficult to determine if the experienced disturbances are due to the brain tumor still being alive, or a side effect of the treatment).[3][4][5] This emphasizes the issue that there are no safe, yet effective, methods for treatment of cancer located in the brain.
In order to fill this knowledge gap, this paper aims to demonstrate the characteristics of the proton irradiation-technique at an hypothetical facility using a cyclotron similar to the one at the 'Skandion Clinic' (currently the Nordic region's only center for proton beam therapy[6]), which can accelerate protons at a kinetic energy of 230 MeV.[7]
Simulations of proton beam therapy in the human brain, using Monte-Carlo, suggest that protons may be accurately used for the treatment of brain tumors.[8][9][10][11] The proton beam is possible to tune such that the stopping range of the protons is optimized to allow for precise targeting of a tumor, with minimal effect on the nearby healthy brain tissue. Appropriate utilization of proton-based therapy (for tumors in the brain) may therefore eliminate necrosis, which in turn could save lives.
2. Materials and Methods
All performed simulations for proton therapy of brain tumors were achieved using the software SRIM (Stopping and Range of Ions in Matter), and it was assumed that the considered cyclotron could accelerate protons at a maximum kinetic energy of 230 MeV. Data from the simulations were then collected and plotted to analyze the stopping range, as well as the transverse spread of the proton beam.
The precise location of a brain tumor may vary extensively, however, it is here taken for granted that the 3-dimensional position of the tumor in the brain is already known. The proton beam can therefore accurately be positioned such that it is transversely pointing directly towards the center of the tumor.
To simulate the circumstances present during brain tumor treatment, a toy-model of the adult human head was constructed within SRIM. Specifically, the layers through which the protons pass to reach the tumor were concretized as: Skin rarr\to Soft (adipose) tissue rarr\to Cranium rarr\to Brain. A specification of the layer widths and their composition is also needed to accurately simulate the situation, the specifics of the model simulated in this paper are seen below in Table 1 (inspired by models presented by [12] and [13]).
Table 1: Density, width, and weighted element composition of different tissues.
Tissue type
Density, "g/cm"^(3)\bf\text{g/cm}^3
Width, "mm"\bf\text{mm}
H
C
N
O
Ca
Na
P
S
Cl
K
Skin
1.09
1.2
0.10
0.204
0.042
0.645
–
0.002
0.001
0.002
0.003
0.001
Soft tissue
1.03
4
0.105
0.256
0.027
0.602
–
0.001
0.002
0.003
0.002
0.002
Cranium
1.61
6
0.05
0.212
0.040
0.435
0.176
0.001
0.081
0.003
–
–
Brain
1.04
50
0.107
0.145
0.022}
0.712
–
0.002
0.004
0.002
0.003
0.002
To modulate the range of the protons it is necessary to add another layer just outside of the head, different widths of this layer will slow down the protons differently and make it possible to stop them at a preferable location (i.e. at the tumor). This layer is here assumed to be made of pure copper, and its specific width should vary depending on how deep into the brain the tumor is.
An illustration of the modeled human head with approximate size relation between the different layers, according to Table 1, is seen in Figure 1 (note that this figure only aims to illustrate the head model, and therefore does not include the copper layer).
Figure 1: Depiction of the layers in the human head through which the protons pass to reach the tumor. (Not to scale; Revised from [12]).
3. Results
To know what width of the copper plate to use, the stopping range of protons in pure copper is investigated. This is achieved by simulating the event in SRIM, and by knowing the energy of the protons. Depending on how deep the tumor is, it is now possible to find an appropriate thickness of the copper plate, such that the protons will stop early enough to not harm any healthy tissue in the brain. Through several simulations, and initially by trail-and-error, it is possible to find a relation between what copper plate width is suitable to use for different tumor positions (depths).
It was found that it takes 55.0 mm copper to completely stop protons with a kinetic energy of 230 MeV. For the protons to reach some distance into the head, the copper plate thickness should therefore be slightly less than 55 mm.
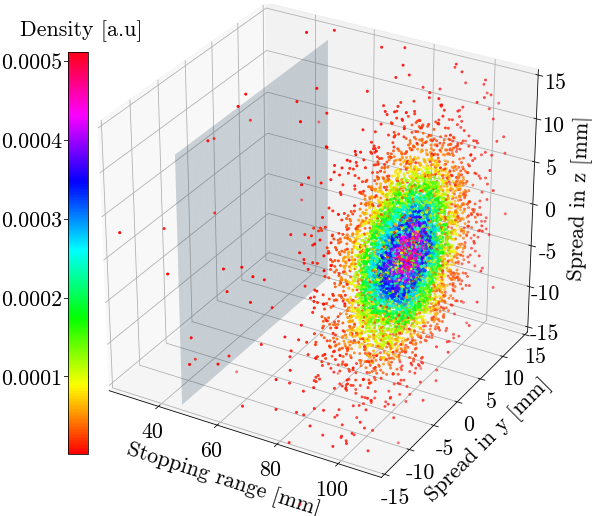
In Figure 2, the stopping range of the protons can be seen. The protons traveled through a 47 mm thick copper plate before they entered the human head. The tumor was assumed to be located at a distance of 50 mm from the surface of the head, i.e. 38.8 mm deep into the brain.
Figure 2: Illustration of proton stopping range in 3 dimensions, where the translucent plane marks the transition between the copper plate and the human head (the protons originate from (0,0,0)). The mediums through which the protons travel are the same as previously showcased in Figure 1 and Table 1, however, they now also travel through a 47 mm thick copper plate. The color map represents the concentration of the protons' stopping points, where red depicts sparse, and blue/purple corresponds to the densest area.
It appears that the densest part of the transverse spread is reaching roughly 10 mm in each direction of the yy -zz plane (parallel to the surface of the head). It is also observed that there is an extra dense area of proton stopping points around the center of the imagined tumor, this area is estimated to have a 5 mm radius. As seen further down in Figure 4, this area also corresponds to the position where the protons will deposit the most energy (excluding the copper plate, which by construction will account for the greatest energy absorption).
However, to properly observe the distribution of how far the protons reach into the head, a top view of Figure 2 is considered, see Fgiure 3.
Figure 3: The figure shows a top view of Figure 2. It is noted that the three main areas are centered around the stopping range of 97 mm, and the most intense area is represented by a sphere of radius 5 mm.
The image reveals a similar pattern of the distribution as when seen from the front. Therefore, it can be concluded that the most intense area of stopping points occupies space in the form of a sphere, with a radius of roughly 5 mm. By considering the yellow area to be significant, the relevant sphere is seen to have a radius of roughly 10 mm.
The energy deposition in different parts of the head is shown in Figure 4, the stopping points from Figure 3 are also included.
Figure 4: Energy deposition and stopping points combined to illustrate how they relate to each other. Note the position of the far-right energy increase in relation to the densest area of proton stopping points.
It is observed that there is a local maximum inside the brain, around the area where the majority of protons stop. A local increase in energy loss is also noticed in the vicinity of the cranium.
The relation between what copper plate width is suitable for the treatment of tumors at different depths into the human head was, by simulated data, found to be according to the linear fit shown in Figure 5.
Figure 5: Linearly fitted data illustrating the relation between proton reach into the head (alternatively tumor depth), and copper plate width. All tumor depth values were simulated with an uncertainty of 1 mm, indicated by error bars.
The linear fit allows for the calculation of which plate width to use depending on the tumor position in the head. The specific relation is given by,
where W_("Copper")W_\text{Copper} is the width of the copper plate in millimeters, and D_("Tumor")D_\text{Tumor} is the depth of the tumor measured in millimeters from the surface of the head (alternatively interpreted as the most occurring stopping range of the protons, measured form the surface of the head).
4. Discussion
Through the simulations in SRIM, it is shown that proton therapy of tumors in the brain is promising for minimizing the damage dealt to healthy tissue. The proton stopping is accurate to the extent of a sphere with a radius of 10 mm, where the densest area of stopping points is concentrated in the volume of a sphere with a radius of just 5 mm. In comparison to the typical tumor with a radius of 10 mm (mean size according to [14], however, radii between 1.5 mm and 33 mm does occur), these numbers are ideal. It would be expected that this accuracy is sufficient enough for the treatment of tumors as small as 5 mm in radius, and the damage of the surroundings should still be minimal.
4.1. Energy Distribution
It was observed that the site-specific energy loss increased in both the area around the cranium and around the area where the majority of protons stopped. The increase around the stopping point is expected due to the higher concentration of protons reaching that area, however, the seemingly abrupt increase around the cranium can likely be explained by the fact that the cranium is much denser than the skin and soft tissue layers.
4.2. The Copper Plate & Small Heads
The other main finding in this study is the relation between copper plate width and proton stopping point. The plot of the data showed a linear behavior, where the error bars also covered the minor fluctuations of the measured data around the linear fit. This relation supplies a reliable tool for calculation of what copper plate width to use during the proton therapy, depending on the tumor location. The data range for tumor depths investigated here covers the majority of the relevant cases since the adult human brain measures roughly a mean radius of 80 mm (according to [15]). However, the linear trend is expected to be almost unchanged for larger distances, that is if the composition of the brain is assumed to be the same throughout the whole brain. Although the transverse spread would intuitively be expected to increase with distance, the effect is less relevant in the small scale that is considered here (at most tens of millimeters), therefore, the effect should be negligible.
However, it should be emphasized that the simulations made in this study only considered the adult human head. For treatment of brain tumors in e.g. children, certain circumstances changes, specifically, the cranium of a child is much thinner than the adult one, even the skin layer and soft tissue layer may differ slightly. Therefore, it should be carefully considered when performing the proton therapy on non-fully developed heads. In other words, it is necessary to perform separate simulations that specifically regard the layer widths in the layout of a children's head, to know what copper plate width to use (note that Eq. [1] would be slightly different). The same cautions should be made regarding the treatment of brain tumors in pets and other animals.
4.3. Other Studies & A General Issue
Other studies such as [16] and [17] have come to the same conclusion about the usefulness of proton-based cancer therapy, especially regarding tumors located in sensitive areas, such as the brain. Furthermore, Newhauser and Zhang, emphasizes in [16] that:
[···] many clinical treatment techniques exploit multiple field directions to enhance the uniformity of tumor coverage and to spare sensitive healthy tissues. In fact, in some cases proton treatments provide inferior skin sparing to photons and/or inferior target coverage, e.g. because of proton beams’ sensitivity to range errors. Nonetheless, beam for beam, proton beams provide excellent tissue sparing [···]
Another point, made by [18], is that even though proton therapy has been shown to minimize healthy tissue damage, there is still an unintentional radiation exposure caused by the circumstances. Particle therapy, in general, includes a beam of charged particles, however, neutron radiation will arise due to nuclear reactions caused by protons. This neutron radiation exposure may in turn increase the risk of developing additional tumors in the future.
5. Conclusions
The findings in this study suggests that proton beam therapy is one of the most promising methods to use for the treatment of brain tumors, due to its limited transverse spread it is suitable for the treatment of the average brain tumor, and accurate controllable stopping range made possible using a copper plate. Even though there exists 'leakage radiation', other radiation-based therapy does not spare healthy tissue to the same extent as proton therapy.
The realized preciseness of proton therapy may well be adapted for the treatment of tumors located elsewhere than in the brain, therefore contributing to overall less harm caused when treating cancer. Further studies can be performed on area-specific tumor treatment, taking into account the layer layout and composition depending on where the tumor is located in the body. Further studies could also include treatment of children's brain tumors, where extra care is taken into the calculation of what copper plate width should be used.
Moreover, one of the main issues that are not solved by proton therapy is the unintentional radiation caused by neutrons. Therefore, more research is needed within this area to achieve a completely harmless method for the treatment of cancer.
To summarize, this paper has emphasized the possibilities made available using proton therapy, and how it may be used to cause minimal damage to healthy tissue when treating brain tumors. The minimization of unintentionally damaged tissue would lower the risk of developing a second tumor caused by the treatment of the first tumor. In turn, this careful treatment of tumors could in the long run relieve the hospital care, and through the smaller risk of re-developing a tumor, it has the potential to save lives.
6. Acknowledgments
I thank the creators of the freeware SRIM, which made this study possible. I also give my sincere thank you to Robert Frost, at the Department of Nuclear Physics at Lund University, for the input.
F. J, E. M, L. F, C. M, M. L, and P. M. et al., Lyon: International Agency for Research on Cancer (2020). ↩︎
J. C. Buckner, P. D. Brown, B. P. O’Neill, F. B. Meyer, C. J. Wetmore, and J. H. Uhm, in Mayo Clinic Proceedings, Vol. 82:10 (Elsevier, 2007) pp. 1271–1286. ↩︎
E. Almhagen, “Development and validation of a scanned proton beam model for dose distribution verification using monte carlo”, (2015). ↩︎
U. Titt, Y. Zheng, O. N. Vassiliev, and W. D. Newhauser, Physics in Medicine & Biology 53, 487 (2007). ↩︎
M. Moteabbed, T. I. Yock, and H. Paganetti, Physics in Medicine & Biology 59, 2883 (2014). ↩︎
L. Widesott, S. Lorentini, F. Fracchiolla, P. Farace, and M. Schwarz, Physics in Medicine & Biology 63, 145016 (2018). ↩︎
O. Ardenfors, A. Dasu, J. Lillhök, L. Persson, and I. Gudowska, Physica Medica 53, 129 (2018). ↩︎
S. B. Jia, M. H. Hadizadeh, A. A. Mowlavi, and M. E. Loushab, Reports of Practical Oncology & Radiotherapy 19, 376 (2014). ↩︎
J. F. Ziegler and J. P. Biersack, SRIM-2008, Stopping power and range of ions in matter (IAEA, 2008). ↩︎
S. Oya, B. Sade, and J. H. Lee, Surgical neurology international 2 (2011). ↩︎
Y. Yan, P. Nunez, and R. Hart, Medical and Biological Engineering and Computing 29, 475 (1991). ↩︎
W. D. Newhauser and R. Zhang, Physics in Medicine & Biology 60, R155 (2015). ↩︎
J. P. Gross, S. Powell, F. Zelko, W. Hartsell, S. Goldman, J. Fangusaro, R. R. Lulla, N. P. Smiley, J. H.-C. Chang, and V. Gondi, Neuro-oncology 21, 934 (2019). ↩︎
W. D. Newhauser and M. Durante, Nature Reviews Cancer 11, 438 (2011). ↩︎
Group Equivariant Convolutional Networks in Medical Image Analysis
Group Equivariant Convolutional Networks in Medical Image Analysis
This is a brief review of G-CNNs' applications in medical image analysis, including fundamental knowledge of group equivariant convolutional networks, and applications in medical images' classification and segmentation.